
http://www.cdc.gov/h1n1flu/update.htm
The 2009 influenza pandemic has spread internationally with unprecedented speed. In past pandemics, influenza viruses have needed more than six months to spread as widely as the new H1N1 virus has spread in less than six weeks.
Novel H1N1 Flu Situation Update
July 31, 2009, 11:00 AM ET
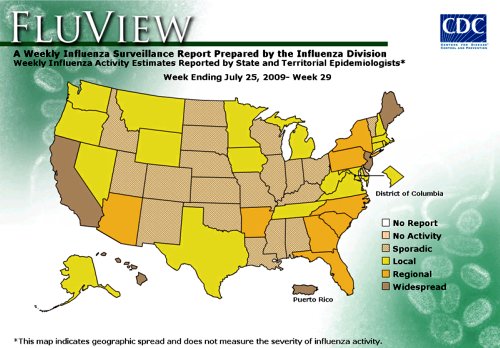
Map: Weekly Influenza Activity Estimates Reported by State and Territorial Epidemiologists
(Activity levels indicate geographic spread of both seasonal and novel influenza A [H1N1] viruses)
(Posted July 31, 2009, 1:30 PM ET, for Week Ending July 25, 2009)
~
**********
*(If your state is now counted in "regions" here is that US map).
~

~
**********
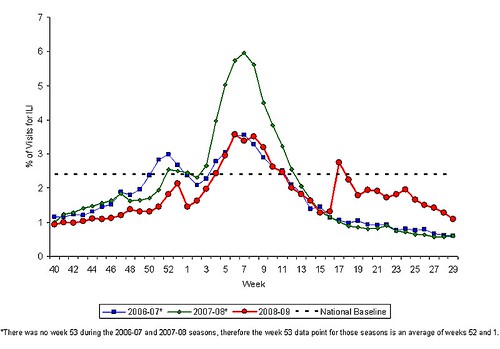
Percentage of Visits for Influenza-like Illness (ILI) Reported by the U.S. Outpatient Influenza-like Illness Surveillance Network (ILINet), National Summary 2008-2009 and Previous Two Seasons
(Posted July 31, 2009, 1:30 PM ET, for Week Ending July 25, 2009)
~
~
~
Changes in reporting requirements for pandemic (H1N1) 2009 virus infection
Pandemic (H1N1) 2009 briefing note 3 (revised)
(From here): http://www.who.int/en/
16 JULY 2009 | GENEVA -- As the 2009 pandemic evolves, the data needed for risk assessment, both within affected countries and at the global level, are also changing.
At this point, further spread of the pandemic, within affected countries and to new countries, is considered inevitable.
This assumption is fully backed by experience. The 2009 influenza pandemic has spread internationally with unprecedented speed. In past pandemics, influenza viruses have needed more than six months to spread as widely as the new H1N1 virus has spread in less than six weeks.
The increasing number of cases in many countries with sustained community transmission is making it extremely difficult, if not impossible, for countries to try and confirm them through laboratory testing. Moreover, the counting of individual cases is now no longer essential in such countries for monitoring either the level or nature of the risk posed by the pandemic virus or to guide implementation of the most appropriate response measures.
Monitoring still needed
This pandemic has been characterized, to date, by the mildness of symptoms in the overwhelming majority of patients, who usually recover, even without medical treatment, within a week of the onset of symptoms. However, there is still an ongoing need in all countries to closely monitor unusual events, such as clusters of cases of severe or fatal pandemic (H1N1) 2009 virus infection, clusters of respiratory illness requiring hospitalization, or unexplained or unusual clinical patterns associated with serious or fatal cases.
Other potential signals of change in the currently prevailing pattern include unexpected, unusual or notable changes in patterns of transmission. Signals to be vigilant for include spikes in rates of absenteeism from schools or workplaces, or a more severe disease pattern, as suggested by, for example, a surge in emergency department visits.
In general, indications that health services are having difficulty coping with cases mean that such systems are under stress but they may also be a signal of increasing cases or a more severe clinical picture.
A strategy that concentrates on the detection, laboratory confirmation and investigation of all cases, including those with mild illness, is extremely resource-intensive. In some countries, this strategy is absorbing most national laboratory and response capacity, leaving little capacity for the monitoring and investigation of severe cases and other exceptional events.
Regular updates on newly affected countries
For all of these reasons, WHO will no longer issue the global tables showing the numbers of confirmed cases for all countries. However, as part of continued efforts to document the global spread of the H1N1 pandemic, regular updates will be provided describing the situation in the newly affected countries. WHO will continue to request that these countries report the first confirmed cases and, as far as feasible, provide weekly aggregated case numbers and descriptive epidemiology of the early cases.
For countries already experiencing community-wide transmission, the focus of surveillance activities will shift to reporting against the established indicators for the monitoring of seasonal influenza activity. Those countries are no longer required to submit regular reports of individual laboratory-confirmed cases to WHO.
Monitoring the virological characteristics of the pandemic virus will be important throughout the pandemic and some countries have well-established laboratory-based surveillance systems in place already for seasonal influenza virus monitoring. Even in countries with limited laboratory capacity, WHO recommends that the initial virological assessment is followed by the testing of at least 10 samples per week in order to confirm that disease activity is due to the pandemic virus and to monitor changes in the virus that may be important for case management and vaccine development.
Updated WHO guidelines for global surveillance reflect in greater detail these recommended changes, in line with reporting requirements set out in the International Health Regulations.
